 In 2010, Michael Gove was appointed to the UK Privy Council, giving him title of “The Right Honorable” for life. “Decisions of the Privy Council are recorded in Orders which have the force of law.”
In 2010, Michael Gove was appointed to the UK Privy Council, giving him title of “The Right Honorable” for life. “Decisions of the Privy Council are recorded in Orders which have the force of law.”
………………………..
Titled UK bureaucrat Mr. Gove imagines that he, among those “gathered round the cabinet table,” had to make the “difficult decision” to order the untitled in the “small, densely populated country” to “sacrifice even more:” “This was not a sacrifice for the “greater good.” It was not a hard decision with arguments on both sides….The “risks” were in fact certainties….All the suffering of lockdown was entirely predictable….Even if you subscribe to the belief that “Sars-Cov-2” is a unique discrete entity (which is far from proven), or that it is incredibly dangerous (which is demonstrably untrue), the lockdown has not worked to, in any way, limit this supposed threat.…The scale of the impact cannot be overstated.” 3/23/21, “Lockdown One Year On–It doesn’t work, it never worked & it wasn’t supposed to work,” Off Guardian, Kit Knightly
…………………………
Nov. 28, 2020, “‘Lockdown was the only way to stop the NHS being broken’ – The Times Weekend Essay,” gov.uk, Cabinet Office, and The Rt Hon Michael Gove MP, Published: 1 December 2020″
“Comment piece from the Chancellor of the Duchy of Lancaster, originally published in the Times on Saturday 28 November 2020.”
“It was a decision none of us wanted to take. But it was a decision none of us could avoid. When ministers met just one month ago to consider whether to introduce a second national lockdown we were presented with a Devil’s dilemma.
We were being asked to impose restrictions on individual liberty which went against every instinct we have had all our adult lives. We would be asking friends and families to avoid each other’s company. We would be closing shops, bars and restaurants, and not just denying people the social contact which defines us as human beings but also suppressing the animal spirit which keeps our economy going. We would be asking millions who had already given up so much to sacrifice even more.
So why did those of us gathered round the cabinet table that Friday afternoon decide that we would, indeed, choose to make November 2020 such a difficult month? For the same reason that Emmanuel Macron in France, Sebastian Kurz in Austria, Micheál Martin in Ireland, Mark Rutte in the Netherlands, Angela Merkel in Germany, Stefan Löfven in Sweden and so many other democratic leaders chose to restrict their people’s freedoms. And for the same reason that the eight political parties in power in devolved administrations have taken similar steps to the UK government. Because the alternative would have been indefensible.
We had to act, as they did, because if we did not
our health service would have been overwhelmed.
That Friday morning I was in Surrey, looking forward to a trip later to an award-winning business in my constituency, the Hogs Back Brewery. But a cloud already hung over my day. I knew that the data coming in from the frontline of the fight against the virus was ominous. So I was not surprised, although I was certainly chilled, by the summons to an action meeting to consider the difficult steps that might now be required. Of course, I’d change my diary: was the meeting tomorrow, or Sunday? No — please get back to London as soon as possible.
That afternoon we were confronted with what would happen to our hospitals if the spread of the virus continued at the rate it was growing.
Unless we acted, the NHS would be broken.
Infections were doubling fast. The number of days taken to see that increase was open to question. But the trend was not. Infection numbers were growing in areas which had previously seen low prevalence. And as the numbers infected increased so, with iron logic, did the numbers in our hospitals. We could not know exactly when, or how late, we could leave it and still have time to pull the handbrake to avoid disaster, but sooner or later our NHS hospitals would be full.
Not just administratively at full stretch. But physically overwhelmed. Every bed, every ward occupied. All the capacity built in the Nightingales and requisitioned from the private sector too. The NHS could, and would, cancel the operations of patients waiting for hip replacements and other routine procedures to free up more beds. But that wouldn’t be enough. The numbers infected with Covid-19 and requiring a bed would displace all but emergency cases. And then even those. With every NHS bed full, the capacity of the health service to treat new emergency cases–people who had suffered serious accidents, heart attacks, strokes–would go.
The questions we asked that afternoon–-and had asked before–were the questions we were to hear everyone ask after we took our decision. Couldn’t NHS capacity have been increased to meet this pressure? Well it had been; the Nightingales had been built, staff redeployed, retired doctors and nurses called to the colours. But while capacity had been, and can be, increased, there is a limit. With the numbers becoming infected and facing hospitalisation doubling, there comes a point where no more flexibility exists. It is difficult to strengthen flood defences when the tsunami is surging towards the shore. Hospitals need doctors and nurses and you can’t double their numbers in a month. And even if you could, you would still need to slow the virus spreading to stop even that capacity being overwhelmed.
Could not more patients be treated at home? And surely improvements in treatment—dexamethasone and non-invasive oxygen support–had made the virus less deadly? Well yes, some patients could be treated at home but the difference could only be made at the margins. And yes, these new treatments reduced mortality. But they relied on patients being in hospital and receiving the treatments from trained professionals. And that was precisely the resource that would run out.
Keeping our hospitals open, available and effective was not just crucial to dealing with Covid-19. It was imperative for the health of the whole nation. But the only way to ensure we can take care of cancer patients, administer radiotherapy and chemotherapy, and help stroke victims and treat heart attacks is by protecting the NHS. And the only way we can do that is by reducing the spread of the virus, thus limiting the number of Covid-19 patients in hospital. Reducing infections is not a distraction from saving other lives, it is a precondition of saving other lives.
And just as we want to reduce Covid-19 infections to save lives, so reducing them is the key to saving the economy.Think for a moment what would happen to our economy if we allowed infections to reach such a level that our NHS was overwhelmed. Would
families seek out crowded bars and buzzing restaurants if they knew
they could be infecting friends and relatives who could not be treated
if they fell ill? Would we flock to the January sales if the doors to
our hospitals were shut? Would investors, entrepreneurs and tourists
make a beeline for Britain if we could not even guarantee the lives and
welfare of our existing citizens? [Is this The Onion?]
All the arguments against lockdown came up against that harsh, brute reality. If this government could not guarantee that the NHS was there for our citizens, it would not just be a political and moral failure. It would mean Covid-19 patients who could be saved would die; cancer patients who could be cured would be lost; thousands in pain would suffer for longer; countless more would lose years of their lives; the economy would grind to a halt, as a population we could not protect sought to save their loved ones; and the world would hang an indelible quarantine sign over our nation’s name.
So we acted. And we did so knowing that the most difficult lesson we had learnt that year is that tougher measures than we would ever want to impose are required to restrict the virus’s spread. The tiers we had in place before the lockdown had not suppressed it sufficiently: they were neither strong enough to reduce social contact sufficiently, nor applied widely enough to contain the virus’s spread. And that is the difficult lesson we cannot unlearn as this lockdown ends.
Thanks to the chancellor’s swift action, millions of people have been helped financially through the dark days of this crisis. Since March, we have provided more than £200 billion in fiscal support. We have extended the furlough scheme to the end of March next year, and businesses that are forced to close can get grants of up to £3,000 a month. For councils, we have also provided an additional £900 million on top of previous funding, to support local economies and communities and fund local healthcare needs.
This coming month brings hope. Vaccines that will defeat the virus are motoring towards regulatory authorisation and distribution. We are seeing strong efficacy rates coming out of the Pfizer/Biontech, Moderna and Oxford/Astrazeneca trials, and the regulator is reviewing both the Pfizer and Oxford vaccines to determine if they reach the required robust standards for quality, safety and effectiveness. The end of the national lockdown means that in all areas shops can reopen, people can go to the gym, hairdressers and beauty services are available again, collective worship can resume and outdoor sports can restart. And, of course, this Christmas, friends and families across the UK can travel to celebrate in each others’ homes.
But for many, these relaxations are cold crumbs of comfort at the start of a long, harsh winter. The new, tougher tiers which cover most of the country still limit social mixing, keep friends apart and hit pubs and bars particularly hard.
Yet they are grimly, inevitably, necessary. The level of infection across the country remains uncomfortably and threateningly high. The pressure on hospitals is still severe: across the UK, about 16,000 beds are filled with Covid-19 patients, which compares with almost 20,000 at the April peak and as low as 740 on September 11. From the current high base, any sharp uptick in infection
could see the NHS under even more severe threat again.
Before the lockdown, the increase in infections was like a tap filling a bath faster and faster with every day that passed. Lockdown first slowed the pace at which the bath was filling up, then stabilised it. Slowly, it has begun to lower the water level. But as we exit this lockdown the level is still high and it would not take too much, or too rapid an increase, for us to risk it overtopping again.
If, however, we can keep the level of infection stable or, even better, falling, and hold out through January and February [2021], then we can be confident that vaccination will pull the plug on the problem. That is why in our Winter Plan we have set out new, stronger tiers. Bluntly, our previous tiers were not as effective as we had hoped. In general, infections continued to rise in Tier 1 and Tier 2 areas and even the bare, basic, old Tier 3 wasn’t enough.These are, of course, uncomfortable truths. Not least for those of us who argued that these measures, on their own, would be enough. But we cannot ignore the evidence. What has worked, however, is the combination of a toughened Tier 3 and widespread community testing. In Liverpool, the mayor Joe Anderson bravely adopted measures above and beyond the old basic Tier 3 and championed mass testing.The result: falling infections, reduced hospitalisations and a smooth transfer to the new Tier 2.
Learning from that experience, we are confident that our new, tougher tiers will have a real impact, and equip us to respond to local conditions–guarding against spread, stemming signs of growth, or bringing a local outbreak back under control so that hospital capacity is not overwhelmed.
Why is it, some ask, that when they come into force on Wednesday, so many areas will be in Tiers 2 and 3, when they entered the lockdown a tier below? Because the level of infection, while stabilising, is simply still too high, and many hospitals remain under pressure. And why is it that we did not take an even more localised approach, and carve up local authorities? Because we are a small, densely populated country where this virus has proven it can spread with ease-so casting the net wide is more effective. And for another reason too, which is that many NHS hospital catchments are expansive, and so to protect our hospitals you need to tackle the virus right across the areas they serve.
The truth, however uncomfortable, sets you free. And these new tiers, alongside the wider deployment of mass testing, have the capacity
to prevent our NHS being overwhelmed
until vaccines arrive.
In politics there is often a readier market for comfortable evasions than uncomfortable truths. Some have argued that you can avoid restrictions on everyday life, let the young in particular go out and about, and build up collective or herd immunity–“Just look at Sweden”.
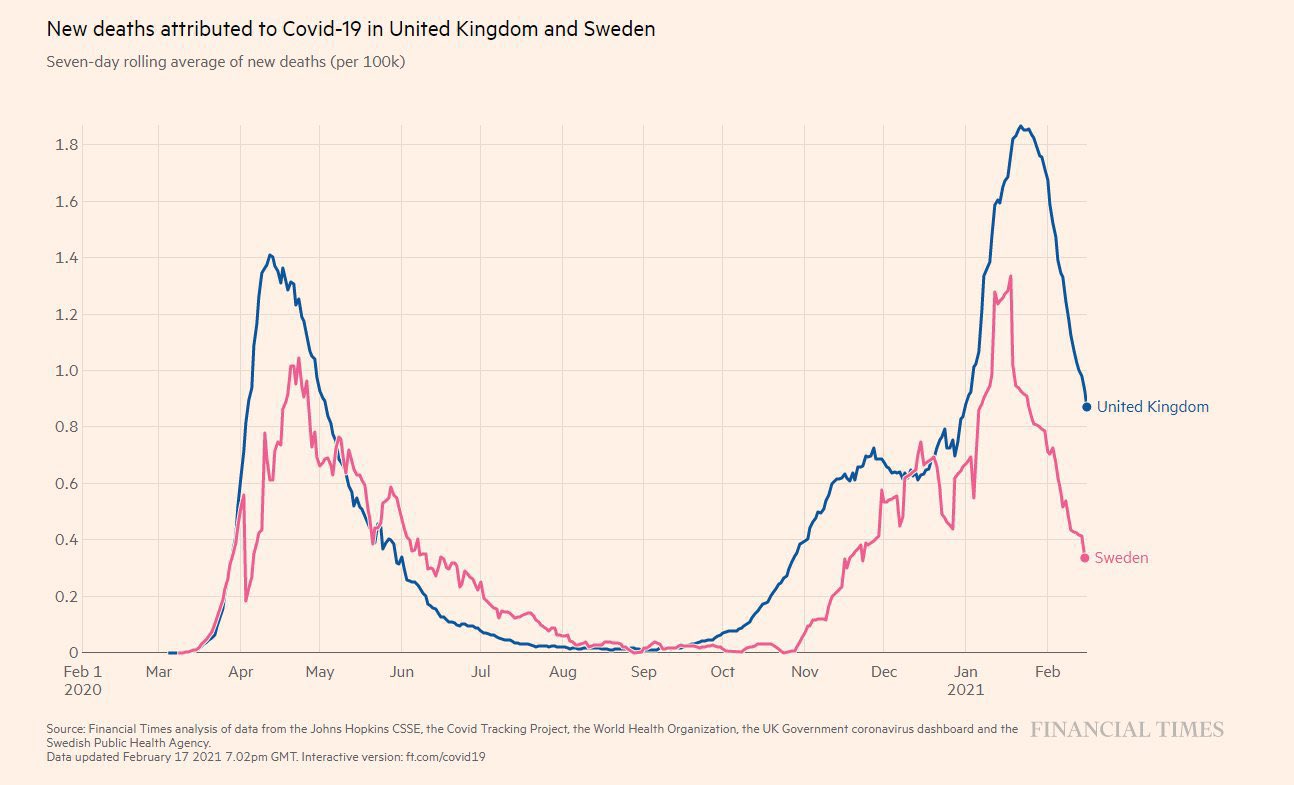 [Graph: As of Feb. 17, 2021 Financial Times analysis, “Covid deaths” in the UK [blue line] (lockdown) and Sweden (no lockdown]
[Graph: As of Feb. 17, 2021 Financial Times analysis, “Covid deaths” in the UK [blue line] (lockdown) and Sweden (no lockdown]
But Sweden, which has in fact always placed restrictions on its population, has found that even the battery of measures it adopted was not enough. Infections rose dramatically in October and early this month, and hospitalisations continue to rise as its government has, reluctantly but firmly, introduced new measures to keep households apart, restrict commerce, stop people visiting bars and restaurants and comprehensively reduce the social contact that spreads infection.
Others have argued, in good faith of course, for a sort of Sweden-that-never-was — for the strict segregation of the most vulnerable while the rest of us go about our business until the pandemic passes. But what would that involve? How, practically, could we ensure that every older citizen, every diabetic, everyone with an underlying condition or impaired immune system was perfectly insulated from all contact with others for months to come? How many are we expected to isolate completely and for how long? Five million? Ten? No visits by carers or medical staff, no mixing of generations, the eviction of older citizens from the homes they share with younger? No country has embarked on this course, with no detailed plan for implementing such a strategy ever laid out.
That is not to deny the course we are on has costs. But those costs are not ones we choose; they are ones we must endure. It is this virus-which in its combination of rapid spread and targeted lethality poses a bigger public health threat than any pandemic since the Spanish flu of 1918-which brings terrible costs. As previous pandemics always have.
And when the country is facing such a national crisis, the truth is that all of us who have been elected to parliament, not just ministers, must take responsibility for difficult decisions. Covid-19 is no respecter of constituency boundaries and the hardships we are facing now are unfortunately necessary to protect every single one of us,no matter where we live. In any analysis of this government’s, or any government’s approach, the cost of lockdown and restrictions cannot be reckoned against the status quo ante, but only against the cost of inaction, or inadequate action,
and the overwhelming of the NHS.
We know now that the costs, significant as they were, generated by our pre-lockdown measures still did not bring us the benefit of a virus under control. We know now, as do other European and western nations, that we can keep the enemy at bay until vaccination turns the tide, but it will be tough. For France, with cafés and restaurants closed across the country until January; for Germany, where even as I write they debate whether even school closures may be necessary; in the US, where Joe Biden, the president-elect, knows he must enter office imposing tougher restrictions to cope with resurgent infections, the need to act is the same. Because the grim calculus of infection is the same. We cannot alter the mathematics, bargain with the virus or evade our responsibilities.
But we can see an end to this. We can end the suffering. Mass testing, vaccination, liberation. But until that liberation comes, we must stand firm. Stand in solidarity with each other. And shoulder the sacrifices required to save the lives of those we love.”
………..
"The original article can be found on the Times’ website here.”
………………………………………..
Added:
As of Jan. 26, 2021, Financial Times analysis, “Comparing “Covid deaths” in California [red line] (lockdown) and Florida (no lockdown):”

………………………………………………..
Added:

Above image, “The Great Reset Fraud,” Strategic Culture

Above, Prince Charles in his “sustainable” Aston Martin converted to run on biofuel, June 2008

No comments:
Post a Comment